

Population Screening and the Identification of Risk in the COSS Model

By Dr Tammy Hand and Associate Professor David MacKenzie
2025. Volume 1. Article 4.
Introduction
We often say that early intervention is only as good as its ability to reach the right young people at the right time. But how do we know who is at-risk of homelessness or other adverse outcomes before a crisis occurs? How can we reliably reach hidden populations of young people who may never come to the attention of teachers, support workers, or service systems until it is too late?
The COSS Model answers this question with a foundational practice: population screening. Drawing on lessons from health and mental health fields, population screening provides a systematic, equitable, and community-wide method to identify risk before harm occurs. In this article, we unpack why population screening is critical to the COSS Model and how it enables a truly preventive approach to youth homelessness.
Population Screening for Risk
Population screening has long been a cornerstone in public health. It is defined as:
Population-based screening is where a screening test is offered systematically to all individuals in the defined target group within a framework of agreed policy, protocols, quality management, monitoring, evaluation and review. Population-based screening is an organised, integrated process where all activities along the screening pathway are planned, coordinated, monitored and evaluated through a quality improvement framework. All of these activities must be resourced adequately to ensure benefits are maximised (for example, breast cancer screening (Standing Committee on Screening 2018).
There has been a growing advocacy for early identification and prevention most often in the special education and health fields (Albers et.al. 2007).
This model of screening has expanded into fields such as special education and youth mental health. Universal screening is often the first step in a tiered prevention strategy, identifying individuals who may require further assessment or support. Importantly, those not identified as at-risk do not receive intervention. This helps to ensure that resourcing is targeted and efficient, without stigmatising young people.
Why Population Screening for Youth Homelessness?
The current homelessness system is largely crisis-oriented, with minimal capacity for identifying and working with young people before homelessness occurs (Hand & MacKenzie 2020; MacKenzie & Hand 2019; MacKenzie & Hand 2020a; MacKenzie & Hand 2020b; MacKenzie et.al. 2020). This means that supports are not offered to most people until they are actually in crisis, with minimal efforts directed at preventing people from becoming homeless in the first place. If early intervention is to be more than a catchphrase, we must be able to detect risk early and reliably.
Effective early intervention for vulnerable young people needs to be able to reach at-risk young people and their families before the onset of crises. To do that, we need a systematic methodology to uncover risk, including hidden risk. This is where universal screening, delivered at a whole-of-cohort or community level, becomes essential.
Teacher/School Staff Referrals Instead of Universal Screening?
Universal screening as a methodology for early identification does involve some additional costs, specialist data analysis, and reporting. It is sometimes asked whether the same result could be achieved through teacher identification and referral?
In a systematic review of school-based programs for the identification of children and young people with mental health difficulties, Anderson et.al. (2019a) conclude that ‘evidence suggests that overall, universal screening may be the most effective method of identification’. They further conclude that combining universal screening with school staff referrals/ identifications ‘shows promise for increasing accuracy of identification’ (Anderson et.al. 2019b).
There is a body of evidence that shows that systematic school-based approaches can identify a greater proportion of children and young people with mental health difficulties, in comparison to less formal processes such as, teacher or parent identification or referrals, or self-referrals (Garland 1995; Eklund et.al. 2009; Scott et.al. 2009; Dowdy et.al. 2016; Keiling et.al. 2014; Schanding & Nowell 2013). In addition, teachers often report to not being equipped to perform such systemic approaches and consistently under-identify early symptoms of various mental health disorders (Candarella et.al. 2008; Brunh et.al. 2014; Cunningham & Suldo 2014).
Problems Relying on Self-Referrals and Direct Referrals
Some current early intervention programs rely on self-referrals and/or referrals from teachers or parents or some other trusted adult. This means that at-risk young people need to be known by those adults/ professionals to be ‘at-risk’. While this may be effective to some extent in some places or programs, the evidence and experience from teachers, in-school welfare professionals, and community-based welfare professionals is that relying on such referrals is problematic for reasons including:
· Many young people are clever at concealing or minimising the ‘problem’, or what is going on at home, to avoid attention by the adults/professionals who want to help them. Young people have more agency and resourcefulness than is often acknowledged.
· Many young people do not display or share what is happening at home until the situation is ‘further along’ which can impact the implementation of interventions in the prevention or early intervention stage/s.
· Bias, whether intentional or unintentional, by the referrer/adult may be an issue. For instance, previous interactions with a vulnerable young person or perceived understanding of situations may cloud or influence an adult’s perception of the young person and their situation and risk status.
Programs and interventions which rely on self-referrals or direct referrals are likely to miss some young people who are at-risk and could benefit from early intervention or prevention support. Of course, clients of quality and evidence-based programs which rely on self-referrals or direct referrals are likely to receive some benefit. However, such programs cannot claim to be working across an entire cohort or community or school as there is no systematic method of identifying those at-risk.
The research is clear: universal screening consistently outperforms referral-only models in identifying at-risk young people. When combined with local knowledge and engagement, it becomes even more powerful.
As such, there needs to be effective and efficient methods to identify at-risk young people which do not rely exclusively on self-identification and/or referral from teachers/schools or other significant adults in the young people’s lives. To overcome such a program or approach flaw, the COSS Model does not rely exclusively on such a referral method but employs a specific universal population screening methodology.
Population Screening Under the Coss Model and the Australian Index Of Adolescent Development Survey
One of the COSS Model foundations is population screening for risk using a series of indicators on the Australian Index of Adolescent Development (AIAD) Survey instrument combined with local knowledge from schools and a brief screening/engagement interview. This methodology allows risk to be rigorously assessed, and a pre-crisis response/s appropriately delivered.
The COSS Model involves a universal multi-stage screening process, see Figure below.
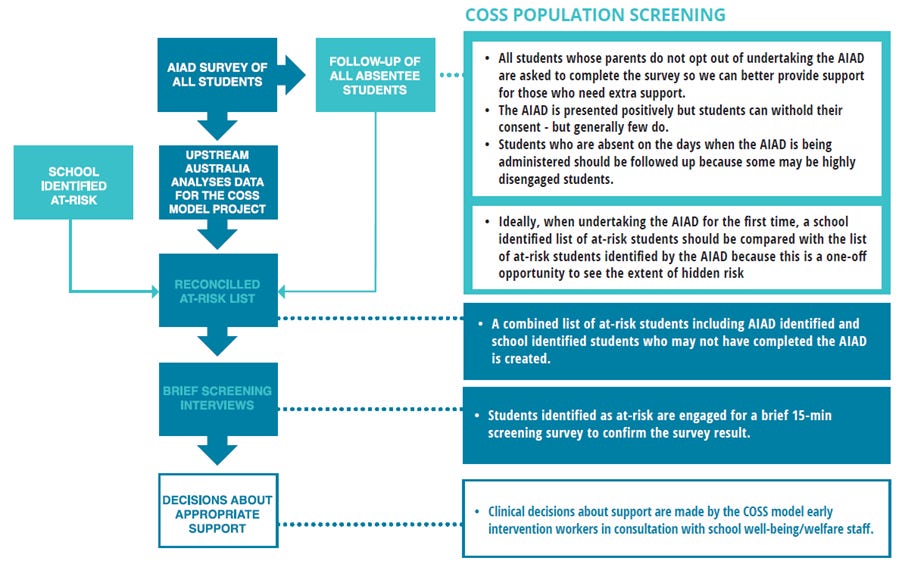
The purpose of the population screening process is to identify young people at-risk so that the COSS early intervention workers can intervene supportively to resolve issues before the onset of full-blown crises. As such, this is a new way that data is being used in a real-world collective impact model, the COSS Model, to inform practice and address the social and educational outcomes for vulnerable young people, including the prevention and early intervention of youth homelessness (MacKenzie & Hand 2020c).
The Australian Index of Adolescent Development (AIAD) Survey, developed by Upstream Australia, plays a key role in the identification of at-risk young people. The AIAD survey includes a range of questions and indicators which cover a range of risk and protective factors (Hand & MacKenzie 2022), including:
· Demographic Variable.
· At-risk of Homelessness Indicator.
· School Disengagement Indicator.
· Psychological Distress Indicator.
· Resiliene Indicator.
· Self-esteem Indicator.
· Connectedness Indicator.
· Anti-social Behaviour Indicator.
The AIAD Survey is administered annually to all students in participating secondary schools. Ideally this should be undertaken in Term 1. A signature advantage of the AIAD Survey and the COSS Model is that it enables hidden populations of risk to be identified - no-one gets left behind.
If data from the indicators in the AIAD Survey suggest that a young person is vulnerable or at-risk, then support and intervention can be delivered pro-actively and before full-blown crises have developed. The COSS methodology allows risk to be rigorously assessed, and a pre-crisis response appropriately delivered in a systematic way. This is ‘indicative prevention’ or ‘targeted prevention’, to use the prevention terminology. A complementary approach (‘selected prevention’), but less efficient, is to identify certain groups in the population that statistically are at significantly higher risk than others and only work with these young people.
The central purpose of the COSS Model is that young people at-risk of homelessness and/or other adverse issues can be identified prior to crises that may occur. For a young person at-risk of homelessness, being identified prior to a homelessness crisis means that they and their family can be supported to resolve any family dysfunction/ issues so that the young person can safely remain living at home and not experience homelessness. Early intervention is predicated on identifying young people at-risk so that the harmful implications can be avoided.
COSS Model practice is that all students in a COSS community participate in the screening process, including completing the AIAD Survey, not only a select ‘at-risk’ group. This enables hidden populations of risk to be identified and then supported, and reduces any potential stigma attached to undertaking the AIAD Survey as ‘everyone completes the survey’.
Why It Matters
This approach fundamentally shifts the paradigm from crisis response to proactive prevention and early intervention. It allows young people and families to access support before risk factors escalate and become entrenched. It also enables systems and services to operate smarter, not just harder.
Conclusion
If early intervention is to live up to its promise, we must stop relying on chance encounters and fragmented referrals. The COSS Model's population screening process is a proven method for identifying risk and intervening early.
It works. And it ensures that no young person is left out or left behind.
References
Albers, C. A., Glover, T. A., & Kratochwill, T. R. (2007). Where are we, and where do we go now? Universal screening for enhanced educational and mental health outcomes [Editorial]. Journal of School Psychology, 45:257-263.
Anderson et al. (2019) cites: Gould, M.S., Marrocco, F.A., Hoagwood, K., Kleinman, M., Amakawa, L & Altschuler, E. (2009). Service use by at-risk youths after school-based suicide screening. Journal of the American Academy of Child and Adolescent Psychiatry, 48:1193–1201.
Anderson, J., Ford, T., Soneson, E., Coon, J., Humphrey, A., Rogers, M., . . . Howarth, E. (2019). A systematic review of effectiveness and cost-effectiveness of school-based identification of children and young people at-risk of, or currently experiencing mental health difficulties. Psychological Medicine, 49(1), 9-19.
Bruhn, A.L., Woods-Groves, S. & Huddle, S. (2014). A preliminary investigation of emotional and behavioral screening practices in K-12 schools. Education & Treatment of Children, 37:611–634.
Caldarella, P., Young, E.L., Richardson, M.J., Young, B.J. & Young, K.R. (2008). Validation of the systematic screening for behavior disorders in middle and junior high school. Journal of Emotional and Behavioral Disorders,16:105–117.
Cunningham, J.M. & Suldo, S.M. (2014). Accuracy of teachers in identifying elementary school students who report at-risk levels of anxiety and depression. School Mental Health, 6:237–250.
Dowdy, E., Dever, B.V., Raines, T.C. & Moffa, K. (2016). A preliminary investigation into the added value of multiple gates and informants in universal screening for behavioral and emotional risk. Journal of Applied School Psychology, 32:178–198.
Eklund, K., Renshaw, T. L., Dowdy, E., Jimerson, S. R., Hart, S. R., Jones, C. N., & Earhart, J. (2009). Early Identification of Behavioral and Emotional Problems in Youth: Universal Screening versus Teacher-Referral Identification. California School Psychologist, 14:89-95.
Garland, A.F. (1995). Pathways to adolescent mental health services: adolescent help-seeking and teacher identification and referral. In Faculty of the Graduate School. US: Yale University.
Hand, T. & MacKenzie, D. (2020) ‘Structures to support collective impact – backbone organisation and multi-levelled working groups’, Concept Brief, Melbourne: Upstream Australia.
Hand, T. and MacKenzie, D. (2022) The Australian Index of Adolescent Development Review 2021-2022: Final Report, Melbourne: Upstream Australia.
Kieling, R.R., Kieling, C., Aguiar, A.P., Costa, A.C., Dorneles, B.V. & Rohde, L.A. (2014). Searching for the best approach to assess teachers’ perception of inattention and hyperactivity problems at school. European Child & Adolescent Psychiatry, 23:451–459.
MacKenzie, D. & Hand, T. (2019). Look beyond crisis accommodation so people like Courtney Herron aren’t homeless in the first place. The Conversation, 10 June 2019. https://theconversation.com/look-beyond-crisis-accommodation-so-people-like-courtney-herron-arent-homeless-in-the-first-place-118182
MacKenzie, D. and Hand, T. (2020a). Redesign of a homelessness service system for young people: A place-based agenda for system change. Parity 33(3):41-44.
MacKenzie, D. and Hand, T. (2020b). 6 Steps towards remaking the homelessness system so it works for young people. The Conversation, 23 April 2020. https:// theconversation.com/6-steps-towards-remaking-the-homelessness-system-so-it-works-for-young-people-136385
MacKenzie, D., Hand, T., Zufferey, C., McNelis, S., Spinney, A. & Tedmanson, D. (2020). Redesign of a homelessness service system for young people, AHURI Final Report No. 327, Australian Housing and Urban Research Institute Limited, Melbourne. https://www.ahuri.edu.au/research/ final-reports/327
Schanding JR, G. T., & Nowell, K. P. (2013). Universal Screening for Emotional and Behavioral Problems: Fitting a Population-Based Model. Journal of Applied School Psychology, 29(1):104-119.
Scott, M.A., Wilcox, H.C., Schonfeld, I.S., Davies, M., Hicks, R.C., Turner, J.B. & Shaffer, D. (2009). School-based screening to identify at-risk students not already known to school professionals: the Columbia suicide screen. American Journal of Public Health, 99:334–339.
Clinical Principal Committee, Standing Committee on Screening. (2018). Population Based Screening Framework. Canberra: Commonwealth of Australia, Department of Health. Page 4. https://www.health.gov. au/resources/publications/population-based-screening-framework?language=en
Short author bio.
Dr Tammy Hand is the Co-founder & Deputy CEO of Upstream Australia. Email: Tammy.Hand@upstreamaustralia.org.au
Associate Professor David MacKenzie is the Co-founder & CEO of Upstream Australia. Email: David.Mackenzie@upstreamaustralia.org.au
Suggested Citation. Hand, T. & MacKenzie, D. (2025). Population Screening and the Identification of Risk in the COSS Model. The Upstreamist, Vol. 1, Article 4.